Introduction
Statins are the most widely prescribed cholesterol-lowering medications in the world, with millions of people taking them daily to protect their heart health. Yet many patients taking statins don’t fully understand how these powerful drugs work, why their doctor prescribed them, or what side effects might occur. This comprehensive statins guide explains everything you need to know about statin medications, from how they work to choosing the right one for your situation.
What Are Statins? Understanding the Most Common Cholesterol Drug
How Statins Work in Your Body
Statins are a class of medications that work by blocking an enzyme in your liver called HMG-CoA reductase. This enzyme is essential for producing cholesterol in your body. By inhibiting this enzyme, statins reduce the amount of cholesterol your liver produces.
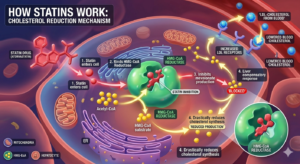
The Science Behind Statins:
When you take a statin, it enters your bloodstream and travels to your liver. There, it binds to HMG-CoA reductase and prevents the chemical reaction that creates cholesterol. As your liver produces less cholesterol, it compensates by pulling more LDL cholesterol from your bloodstream—the “bad” cholesterol that builds up in your arteries.
This process creates multiple benefits:
- Reduced LDL cholesterol (typically 20-60% reduction depending on dose)
- Slightly increased HDL cholesterol (the good kind)
- Reduced triglycerides (especially with higher doses)
- Plaque stabilization in arteries (prevents rupture)
- Anti-inflammatory effects (reduce inflammation in blood vessels)
Timeline of Statin Action:
- Days 1-2: Drug levels build in your system
- Weeks 1-2: Initial cholesterol reduction begins
- Weeks 4-6: Measurable cholesterol improvements visible
- Weeks 8-12: Maximum effectiveness usually achieved
- Ongoing: Benefits maintained as long as you take the medication
Important Note: Statins work while you’re taking them. If you stop taking them, your cholesterol levels typically return to previous levels within weeks.
Why Statins Are Most Prescribed
Statins have become the gold standard for cholesterol management because they:
Are Highly Effective:
- Reduce LDL cholesterol by 20-60% depending on type and dose
- More effective than diet and exercise alone for many people
- Proven track record over decades of use
Have Good Safety Profile:
- Well-tolerated by most patients
- Side effects manageable in most cases
- Serious side effects are relatively rare
Are Affordable:
- Many statins available as generic medications
- Significantly cheaper than newer alternatives
- Good value compared to other cholesterol drugs
Have Strong Evidence:
- Decades of research supporting benefits
- Multiple studies showing cardiovascular protection
- Proven to prevent heart attacks and strokes in high-risk patients
Are Convenient:
- Once-daily dosing typically
- Just a pill to swallow
- No injections or complex administration
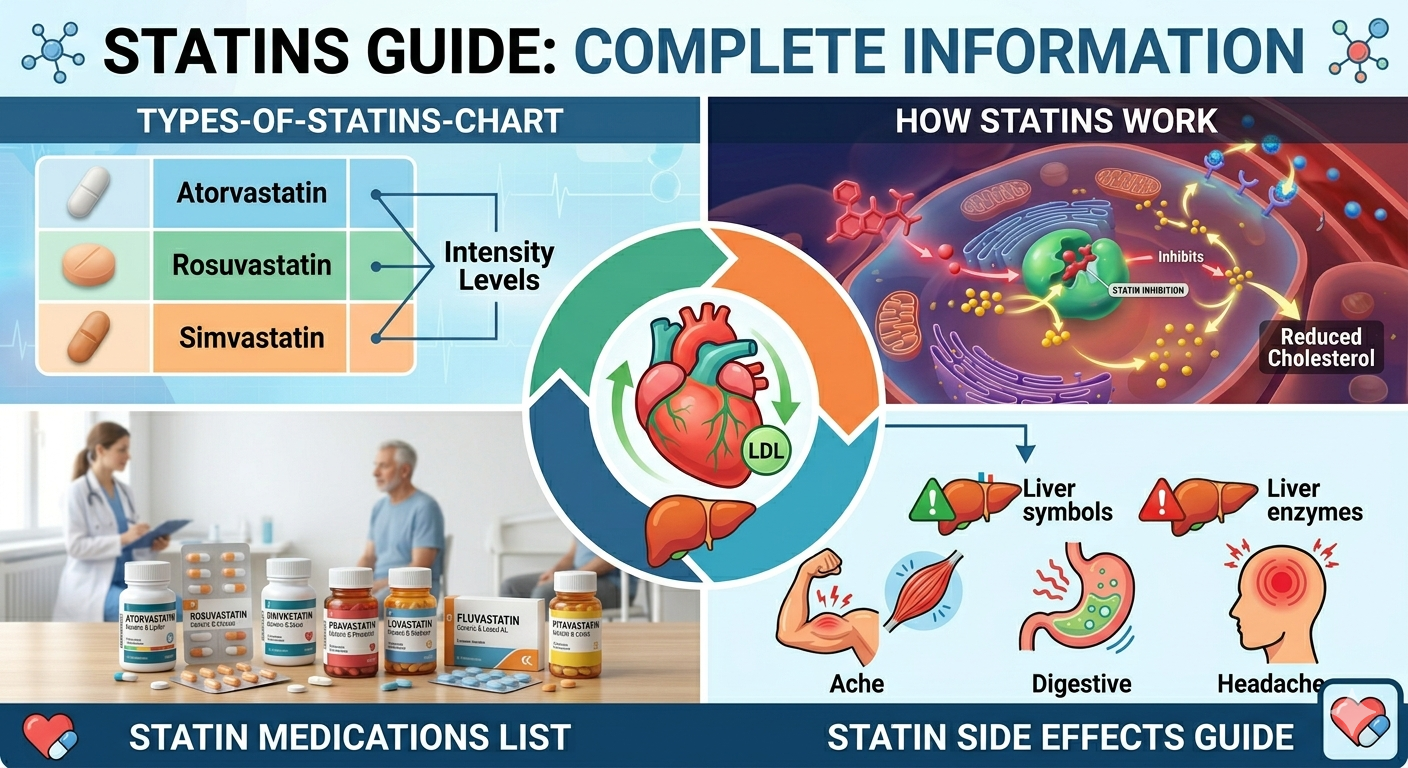
Types of Statins: Complete List & Comparison
Statins are classified by their intensity—how much they lower LDL cholesterol at standard doses.
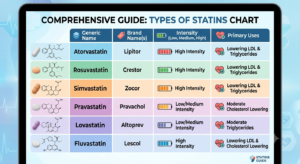
High-Potency Statins
High-potency statins reduce LDL cholesterol by 50% or more at maximum recommended doses.
High-Intensity Statins:
- Atorvastatin 40-80 mg (Lipitor)
- Rosuvastatin 20-40 mg (Crestor)
When Used:
- Very high cholesterol levels
- Previous heart attack or stroke
- Diabetes with multiple risk factors
- Very high-risk patients
Benefits:
- Strongest cholesterol reduction
- Proven cardiovascular benefits
- Options if other statins ineffective
Drawbacks:
- Higher side effect risk
- More drug interactions
- More expensive (especially brand-name)
Moderate-Intensity Statins
Moderate-intensity statins reduce LDL cholesterol by 30-49% at standard doses.
Moderate-Intensity Statins:
- Atorvastatin 10-20 mg (Lipitor)
- Rosuvastatin 5-10 mg (Crestor)
- Simvastatin 20-40 mg (Zocor)
- Pravastatin 40-80 mg (Pravachol)
When Used:
- Most common starting dose
- Moderate cholesterol elevation
- Some cardiovascular risk factors
- Initial treatment before escalating if needed
Benefits:
- Good cholesterol reduction
- Fewer side effects than high-potency
- Good balance of benefit and safety
- Usually sufficient for many patients
Drawbacks:
- May need dose increase for some patients
- Still has side effect potential
- May not be strong enough for very high cholesterol
Low-Intensity Statins
Low-intensity statins reduce LDL cholesterol by less than 30% at standard doses.
Low-Intensity Statins:
- Pravastatin 10 mg
- Simvastatin 10 mg
- Lovastatin (older formulation)
- Fluvastatin
When Used:
- Mild cholesterol elevation
- Elderly patients or those sensitive to medications
- Patients unable to tolerate higher doses
- Starting point before potentially increasing
Benefits:
- Fewest side effects
- Gentle on the system
- Still provides meaningful cholesterol reduction
- Good for sensitive patients
Drawbacks:
- May not be strong enough
- Often requires dose escalation
- Less frequently prescribed today
Generic vs Brand-Name Statins
Generic Statins:
- Same active ingredients as brand-name
- Much cheaper (typically 70-90% less)
- FDA approved as bioequivalent
- Same effectiveness as brand-name
- Examples: Generic atorvastatin (instead of Lipitor)
Brand-Name Statins:
- Original formulation developed by pharmaceutical company
- More expensive but no added benefit
- Same active drug as generic versions
- May have slightly different inactive ingredients (usually doesn’t matter)
Financial Comparison:
- Brand-name atorvastatin: $200-400/month
- Generic atorvastatin: $20-60/month
- Same medication, massive price difference
Doctor’s Recommendation: Most physicians recommend generic statins unless there’s a specific reason for the brand name. Your insurance may also require generic unless medically necessary.
Specific Statin Medications Explained
Atorvastatin (Lipitor)
Overview:
- Most prescribed statin in the US
- Available as generic (very affordable)
- Available in 10, 20, 40, 80 mg doses
- Metabolized by liver (some drug interactions)
How It Works:
- Quickly absorbed and reaches peak levels in 1-2 hours
- Half-life of 14 hours (stays in system ~1 day)
- Works through HMG-CoA reductase inhibition
- Takes effect within weeks
Cholesterol Reduction:
- 10 mg: ~35% LDL reduction
- 20 mg: ~40% LDL reduction
- 40 mg: ~50% LDL reduction
- 80 mg: ~55% LDL reduction
Side Effects:
- Muscle pain (most common): 5-10% of patients
- Liver enzyme elevation: 3-5% of patients
- Nausea, headache: 1-3%
- Serious (rare): Rhabdomyolysis, liver damage
Drug Interactions:
- Strong interaction with certain antifungals
- Interacts with some immunosuppressants
- May interact with macrolide antibiotics
- Always review with pharmacist
Dosing:
- Usually taken once daily
- Can be taken any time of day
- With or without food
- Evening dosing slightly more effective (more cholesterol produced at night)
Pros:
- Most research available
- Generic available
- Very affordable
- Very effective
- Good tolerability for most
Cons:
- Muscle side effects common
- Some drug interactions
- May need dose adjustment in liver disease
Rosuvastatin (Crestor)
Overview:
- Newer statin than atorvastatin
- Highly potent (strongest cholesterol reduction)
- Available in 5, 10, 20, 40 mg doses
- Less hepatic metabolism (fewer drug interactions)
How It Works:
- Slower absorption (peak levels in 3-5 hours)
- Longer half-life: 19 hours
- Long-lasting effect in body
- Highly selective for liver
Cholesterol Reduction:
- 5 mg: ~45% LDL reduction
- 10 mg: ~50% LDL reduction
- 20 mg: ~55% LDL reduction
- 40 mg: ~60% LDL reduction
Side Effects:
- Muscle pain: 3-5% (less than atorvastatin)
- Liver enzyme elevation: 1-3%
- Protein in urine (rare): monitor if kidneys weak
- Serious (rare): Rhabdomyolysis, severe myositis
Drug Interactions:
- Fewer interactions than atorvastatin
- Still avoid certain antifungals
- Safer with many antibiotics
- Good option for those on multiple medications
Dosing:
- Once daily, any time
- With or without food
- Evening dosing slightly more effective
- Starting dose usually 5-10 mg
Pros:
- More potent (stronger cholesterol reduction)
- Fewer drug interactions
- Less hepatic metabolism
- Good for those on multiple drugs
- Lower muscle pain rates
Cons:
- More expensive than atorvastatin
- Generic recently available (still expensive)
- Not necessarily needed for all patients
- May increase kidney-related side effects
Simvastatin (Zocor)
Overview:
- Older statin (used since 1988)
- Available as generic
- Available in 10, 20, 40 mg doses
- Good cholesterol reduction at moderate doses
How It Works:
- Prodrug (becomes active in liver)
- Peak levels in 1-3 hours
- Half-life of 2 hours (but effects last longer)
- Active metabolites have longer half-life
Cholesterol Reduction:
- 10 mg: ~25% LDL reduction
- 20 mg: ~35% LDL reduction
- 40 mg: ~41% LDL reduction
- 80 mg: ~48% LDL reduction (rarely used)
Side Effects:
- Muscle pain: 5-10%
- Liver enzyme elevation: 1-3%
- Headache, nausea: 1-2%
- Similar to atorvastatin profile
Drug Interactions:
- More interactions than atorvastatin
- Cannot use with certain antifungals
- Interacts with many antivirals
- Requires careful medication review
Dosing:
- Usually taken in evening
- Evening dosing very important
- With or without food
- Typical starting dose 20-40 mg
Pros:
- Very affordable generic available
- Effective at moderate doses
- Long track record of safety
- Well-tolerated by most
Cons:
- More drug interactions
- Cannot go above 40 mg safely with certain drugs
- More restrictive due to interactions
- Less strong than newer statins
Pravastatin (Pravachol)
Overview:
- One of earlier statins (used since 1991)
- Available as generic
- Available in 10, 20, 40, 80 mg doses
- Hydrophilic (water-soluble)
How It Works:
- Different structure than other statins
- Hydrophilic (doesn’t cross membranes as easily)
- Active immediately (not a prodrug)
- Minimal hepatic metabolism
Cholesterol Reduction:
- 10 mg: ~20% LDL reduction
- 20 mg: ~25% LDL reduction
- 40 mg: ~32% LDL reduction
- 80 mg: ~37% LDL reduction
Side Effects:
- Muscle pain: 2-5% (less than others)
- Liver enzyme elevation: 1%
- Headache: 1-2%
- Generally very well-tolerated
Drug Interactions:
- Minimal hepatic metabolism
- Very few drug interactions
- Good choice for those on multiple drugs
- Safe with most medications
Dosing:
- Usually once daily
- Can take any time of day
- With or without food
- Timing doesn’t affect effectiveness
Pros:
- Very few drug interactions
- Excellent tolerability
- Good for elderly and complex patients
- Generic very affordable
- Minimal side effects
Cons:
- Less potent than atorvastatin/rosuvastatin
- May need higher doses
- Less commonly prescribed today
- Older statin (less research)
Other Statins
Lovastatin (Mevacor):
- One of first statins developed
- Rarely prescribed today
- Available as generic
- Most interactions of all statins
Fluvastatin (Lescol):
- Least potent statin
- Rarely used in modern practice
- Available as generic
- Few drug interactions
- Good for very sensitive patients
Pitavastatin (Livalo):
- Newer option
- Very potent
- Minimal hepatic metabolism
- Not yet widely used
Statin Benefits: Why Doctors Prescribe Them
Cholesterol Reduction Benefits
The primary benefit of statins is their effectiveness at lowering cholesterol.
LDL Cholesterol Reduction:
- Average 20-55% reduction depending on statin type and dose
- More reduction with higher potency statins
- Response varies by individual (genetic factors)
- Can reduce LDL to target levels in most patients
HDL Cholesterol Increase:
- Modest increase of 2-10% typically
- More with certain lifestyle changes combined
- Even small increases help
- Very important for cardiovascular health
Triglyceride Reduction:
- 10-20% reduction typical
- More with higher doses
- Especially effective in combination with diet changes
- Important for those with metabolic syndrome
Total Cholesterol Reduction:
- 20-30% reduction typical
- Depends on baseline and statin choice
- Results visible within 4-6 weeks
- Maximum benefit at 8-12 weeks
Cardiovascular Protection
Beyond just lowering cholesterol, statins provide direct cardiovascular protection.
Heart Attack Prevention:
- Reduce heart attack risk by 30-40% in high-risk patients
- Prevention is proven in numerous studies
- Benefit increases with duration of use
- Most dramatic benefit in those with existing heart disease
Stroke Prevention:
- Reduce stroke risk by 20-30%
- Benefits seen across different stroke types
- Protective effect increases over time
- Especially beneficial in those with cardiovascular disease
Plaque Stabilization:
- Stabilize existing plaque in arteries
- Prevent plaque rupture (which causes heart attacks)
- Anti-inflammatory effects help
- Can slow progression of atherosclerosis
Arterial Function:
- Improve endothelial function
- Better blood vessel flexibility
- Reduce inflammation in blood vessel walls
- Improve blood flow overall
Additional Health Benefits
Beyond cholesterol and heart protection, emerging research shows other benefits.
Anti-Inflammatory Effects:
- Reduce inflammation throughout body
- May help with various inflammatory conditions
- Benefits for those with chronic inflammation
- Could have broader health impacts
Bone Health:
- Some evidence of improved bone density
- May reduce fracture risk in some populations
- More research needed
- Particularly interesting for elderly patients
Cognitive Benefits:
- May help maintain cognitive function
- Conflicting research on dementia prevention
- Cholesterol important for brain function
- Too-low cholesterol potentially problematic
Cancer Prevention:
- Mixed evidence in research
- Some studies show slight reduction in certain cancers
- Other studies show no benefit
- Not a primary reason to take statins
Statin Side Effects: What You Need to Know
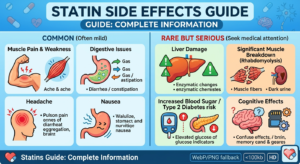
Common Side Effects
Most patients tolerate statins well, but some experience side effects.
Muscle Pain (Myalgia):
- Most common side effect: 5-10% of patients
- Usually mild and manageable
- Ranges from minor aches to severe pain
- Can affect any muscle group
- Often resolves if you continue medication
- May improve by changing statin type
What Causes It:
- Statin’s effect on muscle metabolism
- Individual genetic sensitivity
- Drug interactions
- Dehydration
- Intense exercise
- Thyroid problems (can increase risk)
Managing Muscle Pain:
- Continue medication (often improves)
- Switch to different statin
- Reduce dose
- Take CoQ10 supplement (some evidence)
- Increase hydration
- Reduce intense exercise temporarily
- Wait 8-12 weeks (often improves)
Liver Enzyme Elevation:
- Increases in 1-3% of patients
- Usually mild
- Rarely causes actual liver damage
- Monitored with blood tests
- Usually reversible if medication stopped
What Causes It:
- Statin’s metabolism in liver
- Higher doses increase risk
- Drug interactions increase risk
- Pre-existing liver disease increases risk
When to Worry:
- Enzyme elevation usually temporary
- Often stabilizes while continuing medication
- Significant elevations (3x normal) warrant stopping
- Return to normal upon stopping statin
- Usually can try different statin
Other Common Side Effects:
- Headaches: 1-3% of patients
- Nausea or upset stomach: 1-3%
- Constipation: 1-2%
- Fatigue: 1-2%
- Diarrhea: 1-2%
- Skin rash: <1%
Management of Common Side Effects:
- Usually improve over time
- Often mild enough to tolerate
- Switching statins may help
- Timing of dose can help
- Usually reversible if stopped
Serious Side Effects
Serious side effects are rare but important to know about.
Rhabdomyolysis (Severe Muscle Breakdown):
- Extremely rare: 1-10 per 100,000 patients
- Serious and potentially life-threatening
- Muscle breakdown releases myoglobin
- Can damage kidneys
- Caused by statin’s muscle effects
Warning Signs:
- Severe unexplained muscle pain
- Muscle weakness or swelling
- Dark urine (indicates myoglobin in urine)
- Fever
- Unusual fatigue
If Suspected:
- Stop taking statin immediately
- Seek emergency medical care
- Blood tests needed immediately
- Hospitalization may be required
Risk Factors for Rhabdomyolysis:
- Very high doses
- Drug interactions (especially certain antifungals)
- Kidney disease
- Untreated hypothyroidism
- Previous statin intolerance
- Very intense exercise
Liver Damage (Hepatotoxicity):
- Extremely rare
- Usually reversible
- More common at higher doses
- Risk factors: pre-existing liver disease
Warning Signs:
- Yellowing of skin/eyes (jaundice)
- Dark urine
- Pale stools
- Severe abdominal pain
- Severe nausea/vomiting
If Suspected:
- Contact doctor immediately
- Stop taking medication
- Blood tests needed
- Liver function monitoring essential
Cognitive Side Effects:
- Memory loss reports (very rare)
- Confusion (rare)
- Reversible upon stopping medication
- Controversial (not proven in all studies)
- Most studies don’t show cognitive impairment
Muscle Myositis (Serious Muscle Inflammation):
- Different from simple myalgia
- Inflammation of muscle tissue
- Requires medical attention
- Can progress if not stopped
- Reversible when medication stopped
Managing Side Effects
If You Develop Side Effects:
- Don’t automatically stop taking it
- Many side effects improve over time
- Body may adjust (weeks to months)
- Stopping may not be necessary
- Contact your doctor
- Describe symptoms in detail
- Discuss severity
- Don’t self-adjust dose
- Professional guidance important
- Possible solutions:
- Wait longer (symptoms may resolve)
- Lower the dose
- Switch to different statin
- Change timing (morning vs evening)
- Add medication (for side effect)
- Stop temporarily, retry later
- Add CoQ10 supplement
- Improve hydration
- Prevention strategies:
- Stay well hydrated
- Don’t do intense exercise immediately after starting
- Avoid drug interactions
- Report all medications to doctor
- Get liver function monitored
- Regular muscle symptom checks
Who Should Take Statins?
Statin Guidelines and Recommendations
Major medical organizations provide guidance on who should take statins.
American Heart Association Guidelines:
Definitely Consider Statins:
- Existing coronary artery disease
- Previous heart attack or stroke
- Diabetes (especially with risk factors)
- LDL cholesterol 190+
- Age 40-75 with diabetes and LDL 70+
- Age 40-75 with 10-year heart disease risk 7.5%+
Possibly Consider Statins:
- Age 40-75 with risk factors
- Age 75+ with certain risk factors
- Family history of early heart disease
- Multiple risk factors combined
May Not Need Statins:
- Young with no risk factors
- Normal cholesterol naturally
- Low cardiovascular risk
- No family history
Canadian Guidelines:
- More conservative than US
- Focus on established disease
- Risk assessment for primary prevention
European Guidelines:
- Even more conservative approach
- Higher thresholds for starting
- Focus on actual cardiovascular disease
Risk Factors for Statin Use
Strong Risk Factors (Likely to Need Statins):
- Diabetes
- Smoking
- High blood pressure
- Family history of early heart disease
- Previous cardiovascular event
- Obesity
- Sedentary lifestyle
- Age (older = higher risk)
Moderate Risk Factors:
- Metabolic syndrome
- Chronic kidney disease
- Elevated inflammation
- Stress
- Sleep apnea
Calculate Your Risk:
- Online calculators available
- Take family history into account
- Consider all factors together
- Discuss with doctor
When Statins May Not Be Right
Reasons to Avoid or Reconsider Statins:
- Pregnancy or planning pregnancy
- Severe muscle disease history
- Serious liver disease
- Extremely high rhabdomyolysis risk
- Severe side effects intolerance
- Previous serious statin reaction
- Personal preference (after discussion)
Situations Requiring Caution:
- Kidney disease (dose adjustment needed)
- Hypothyroidism (increase rhabdomyolysis risk)
- Taking multiple interacting drugs
- Alcohol abuse
- Age 75+ (discussion about benefits needed)
Statins vs Alternative Treatments

Statins vs Diet and Exercise
The Ideal Approach: Statins + diet + exercise is most effective
Diet Alone:
- Can reduce cholesterol 10-15%
- May be sufficient for mild elevations
- Takes weeks to months for results
- Requires strict adherence
- Difficult to maintain long-term
Exercise Alone:
- Reduces cholesterol 5-10%
- Increases HDL 3-9%
- Supports weight loss
- Provides cardiovascular benefits
- Takes consistent effort
Combined Diet + Exercise:
- Can reduce 15-25% potentially
- Synergistic effects
- Addresses multiple risk factors
- Requires significant lifestyle change
- Many people can’t achieve/sustain
Statins Alone (no lifestyle changes):
- 20-55% LDL reduction
- Works without lifestyle changes
- Easier compliance
- But misses other benefits of exercise/diet
Statins + Diet + Exercise (IDEAL):
- Up to 50-70% improvement potential
- Addresses multiple factors
- Weight loss easier with support
- Exercise benefits beyond cholesterol
- Diet improves overall health
- Medication ensures consistency
Statins vs Other Medications
PCSK9 Inhibitors (Newer alternative):
- Even stronger cholesterol reduction
- 50-70% additional reduction beyond statins
- Expensive (thousands per month)
- Injectable (usually)
- For statin-intolerant or very high-risk
- Not first-line treatment
Ezetimibe:
- Blocks cholesterol absorption
- 15-20% LDL reduction
- Often combined with statins
- Less effective than statins alone
- Fewer side effects
- Good combination therapy
Bile Acid Sequestrants:
- Older medication class
- 15-30% reduction
- More side effects (GI distress)
- Fewer interactions than statins
- Rarely used alone today
- Sometimes used with statins
Fibrates:
- Focus on triglycerides, not LDL
- 20-50% triglyceride reduction
- Modest LDL effects
- More side effects
- For high triglycerides specifically
- Not primary cholesterol treatment
Niacin:
- Increases HDL significantly
- Lowers LDL and triglycerides
- Significant side effects (flushing)
- Difficult to tolerate
- Rarely prescribed today
- Once popular, now less common
Comparison: Statins are most effective and best-tolerated for most patients. Other medications serve specific purposes (very high risk, intolerance, specific profiles).
Natural Alternatives
Plant Sterols/Stanols:
- Reduce cholesterol 6-15%
- Found in foods or supplements
- Generally safe
- Requires consistent intake
- Not sufficient alone
Red Yeast Rice:
- Contains statin-like compounds
- Unregulated (varying potency)
- Quality concerns
- May have statin side effects
- Not FDA-regulated
- Not recommended alone
Fish Oil Omega-3s:
- Reduce triglycerides (20-30%)
- Modest LDL effects
- Generally safe
- Requires high doses
- May increase bleeding risk
Garlic:
- Modest cholesterol reduction
- Requires very high amounts
- Results inconsistent
- Generally safe
- Not sufficient alone
Soluble Fiber:
- 5-10% cholesterol reduction
- Dietary approach
- Very safe
- Helps overall health
- Works best combined with other approaches
Exercise + Diet:
- Discussed above
- Most important lifestyle factors
- Can achieve 15-25% improvement
- Should ALWAYS be done
- Sometimes sufficient alone
Statin Dosage, Interactions & Monitoring
How to Take Statins
Dosing Basics:
- Usually once daily
- Dose depends on statin type and cholesterol level
- Start low, increase if needed
- Standard doses are proven effective
When to Take:
- Most effective in evening (cholesterol produced at night)
- Some can be taken anytime
- Consistency is important
- Food doesn’t affect most (vary by statin)
Important Rules:
- Take exactly as prescribed
- Don’t adjust dose yourself
- Regular monitoring needed
- Don’t stop without doctor approval
- Set reminder if needed
Missed Doses:
- Take as soon as you remember
- Don’t double up next day
- Continue regular schedule
- Skip if almost time for next dose
Drug Interactions
Major Interactions to Avoid:
With Atorvastatin (Lipitor):
- Ketoconazole and similar antifungals
- Certain protease inhibitors
- Erythromycin and clarithromycin (antibiotics)
- Diltiazem (heart medication)
- Some grapefruit juice
With Simvastatin (Zocor):
- More interactions than atorvastatin
- Ketoconazole and antifungals (contraindicated above 40mg)
- Protease inhibitors
- Certain antibiotics
- Verapamil and diltiazem
- Grapefruit juice (significant)
With Rosuvastatin (Crestor):
- Fewer interactions overall
- Ketoconazole (high dose caution)
- Some antivirals
- Cyclosporine
- Generally safer than simvastatin
With Pravastatin (Pravachol):
- Very few interactions
- Minimal hepatic metabolism
- Generally safe with other drugs
- Best for those on multiple medications
Grapefruit Juice Warning:
- Inhibits enzyme that metabolizes statins
- Increases statin levels significantly
- Can increase side effect risk
- Avoid with certain statins
- Some have less interaction
- Safe with pravastatin
Always Tell Your Doctor:
- All medications (including OTC)
- All supplements
- All herbal products
- Any new medications
- Before starting anything new
Monitoring Your Health
Before Starting Statins:
- Blood test for liver function (AST, ALT, bilirubin)
- Blood test for kidney function (creatinine)
- Cholesterol panel
- Glucose (if diabetic)
- Document any muscle problems
While Taking Statins:
First 6-8 Weeks:
- Initial dose adjustment period
- Monitor for side effects
- Repeat cholesterol test at 4-6 weeks
- Liver function test may be repeated
- Follow-up doctor visit
Ongoing Monitoring:
- Cholesterol test every 6-12 months (after stable)
- Liver function annually (or as recommended)
- Report any new muscle symptoms
- Regular doctor visits
- Blood pressure checks
- Kidney function monitoring (if at risk)
Self-Monitoring:
- Note any muscle pain
- Track energy levels
- Watch for yellowish skin/eyes
- Monitor digestion
- Note any cognitive changes
- Keep symptom diary
When to Contact Doctor:
- New muscle pain or weakness
- Severe fatigue
- Dark urine
- Yellowing of skin/eyes
- Severe abdominal pain
- Mental changes
- Any concerning symptoms
FAQs About Statins
Q: Can I stop taking statins once my cholesterol is normal? A: Usually not. Cholesterol returns to previous levels when you stop. Long-term use typically needed. Discuss with your doctor.
Q: Are statins safe for long-term use? A: Yes, for most people. Decades of research support safety. Regular monitoring important. Benefits usually outweigh risks.
Q: Do I need to take statins forever? A: For most people with indications, yes. Statins work while taking them. Life-long maintenance usually needed for cardiovascular protection.
Q: Can I take statins with other medications? A: Usually yes, but drug interactions possible. Always tell doctor about all medications. Some combinations should be avoided or monitored.
Q: Will statins prevent heart attack/stroke completely? A: Not completely, but significantly reduce risk (by 30-40% typically). Other risk factors still matter. Combined approach most effective.
Q: Are there any natural statins? A: Red yeast rice contains statin-like compounds, but unregulated. Prescription statins are safer and more reliable.
Q: Can muscle pain from statins be prevented? A: Not always, but adequate hydration and vitamin D help. CoQ10 may help some. Avoid intense exercise initially.
Q: How long until statins lower cholesterol? A: Initial reduction within 1-2 weeks. Measurable reduction at 4-6 weeks. Maximum effect at 8-12 weeks.
Q: Are generic statins as good as brand-name? A: Yes, same active ingredient. FDA-approved as equivalent. Equally effective and safe.
Q: Can women take statins while pregnant? A: No, statins should not be taken during pregnancy. Cholesterol important for fetal development. Stop statin if pregnant.


Leave a Reply